Medical Therapy for Hair Loss
 Accurate diagnosis is a prerequisite for the effective treatment of alopecia, or hair loss. Causes of alopecia that may mimic simple, familial-inherited hair loss must be ruled out first. Once this is accomplished through a physician’s consultation and physical exam (and possibly simple laboratory studies) the objectives of stopping hair loss and promoting re-growth may be addressed.
Accurate diagnosis is a prerequisite for the effective treatment of alopecia, or hair loss. Causes of alopecia that may mimic simple, familial-inherited hair loss must be ruled out first. Once this is accomplished through a physician’s consultation and physical exam (and possibly simple laboratory studies) the objectives of stopping hair loss and promoting re-growth may be addressed.
The goal is to slow the rate of hair loss and/or to reverse the hair miniaturization process. Currently, two medications have been approved by the U.S. FDA for these purposes: topical minoxidil and oral finasteride.
Topical 2-5% minoxidil (Rogaine®) lengthens the time that hairs remain in growth phase, enlarges miniaturized follicles, and increases blood flow to follicles. Peak hair growth is seen after 26-52 weeks, with the crown (or vertex) of the scalp showing the best response and the frontal area the least. Although 5% minoxidil is superior to 2% in increasing hair count and hair weight for male pattern baldness, adverse dermatologic effects, most commonly scalp irritation, are more common with the 5% solution. Currently, only the 2% strength is FDA approved for use on women. Cessation of treatment results in reversal of the positive effect within 4-6 months.
Finasteride (Propecia® or Proscar®) inhibits the enzyme involved in converting testosterone to its metabolite, DHT. When taken properly, clinical trials conducted over a 5 year period demonstrated a slowing of hair loss and increased hair counts in a percentage of men. Again, the best response was seen in the crown (or vertex) of the scalp and the least in the frontal area.
It is important that you first consult with a physician prior to beginning oral finasteride therapy. It has been shown to be ineffective in postmenopausal women and is known to cause damage to the fetus of pregnant women. Side effects in men are infrequent, affecting less than 2% of patients. They are reversed after discontinuation of the drug and often resolve during continued treatment. It is also important to inform your physician if you are taking this medication as it may alter the results of various screening tests (e.g. PSA test).
Topical Hair Blends
For Men
The systemic impact of topical finasteride was published in a 2014 article in the Int’l Jour of Clinical Pharmacology.
1) SERUM FINASTERIDE Levels with TOPICAL versus ORAL form.
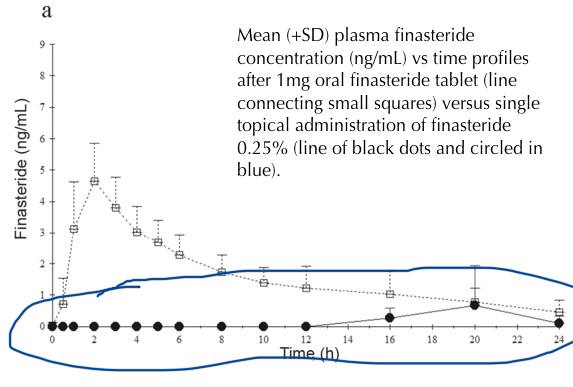 The finasteride levels found in the serum (blood) of patient who used 0.25% topical finasteride once daily were well below the assay’s ability to detect and quantify at nearly every point (circled in blue). The spike in serum finasteride levels of patients taking the pill can be seen above.
The finasteride levels found in the serum (blood) of patient who used 0.25% topical finasteride once daily were well below the assay’s ability to detect and quantify at nearly every point (circled in blue). The spike in serum finasteride levels of patients taking the pill can be seen above.
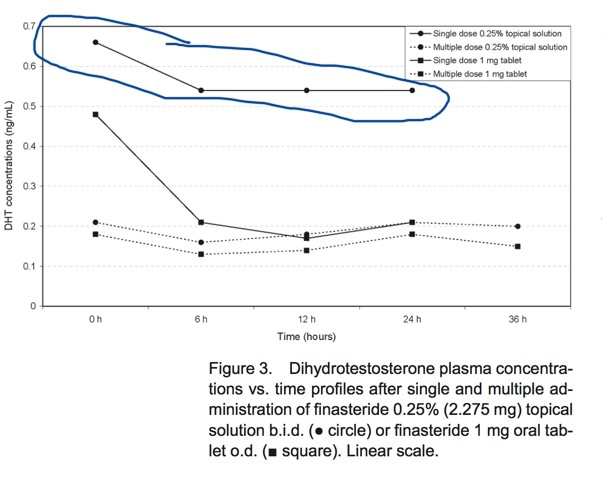
2) SERUM DHT levels with TOPICAL versus PILL form.
Once-a-day use of the 0.25% topical finasteride resulted in much a less severe decrease in DHT plasma levels (19%) that those seen in patients using the pill once a day (70%) or twice daily use of either topical or pill form. Our blend (circled in blue) uses a lower percentage of finasteride than that used in this study and our patients only use the blend once (not twice) daily.
3) No significant change in serum testosterone levels detected with either treatment.
4) A follow-up study showed the topical solution reduces scalp DHT levels by about 70%.
Despite these findings, this alternative to the Propecia pill is not necessarily for everyone. Safety profiles of topical finasteride have not been properly investigated at this stage.
For Women
Topical spironolactone 1% was effective in promoting hair growth in a clinical study with 60 women by reducing enzyme activity in the biosynthesis of testosterone at the scalp level. Unlike what is commonly seen when using the oral form of spironolactone, no hormonal side effects were observed.
Topical 17alpha-Estradiol (0.025%) when used daily for 4 to 8 months produced a statistically-significant increase in hair counts and diameter from baseline in a 53-women clinical trial. Again, no side effects were observed (reference).
Melatonin’s strong anti-oxidant properties may counter the oxidative stressors associated with hair loss. Six months of daily topical Melatonin (0.1%) use generated more anagen (growth phase) hairs in the crown/vertex of the scalp in a 40-women clinical trial compared with a control group. While plasma melatonin levels were slightly elevated, they did not exceed the physiologic night peak (reference).
Minoxidil enhances the thickness of hair and increases the percentage of hairs in the anagen (growth) phase. When combined with Retinol (a derivative of vitamin A) on a daily basis, there is an additive effect on the length and thickness of hair follicles.
Medicated Shampoo
While numerous cosmetic products claim to promote hair growth, few have been investigated with rigorous controlled studies. Two topical elements occasionally found in shampoos that have demonstrated efficacy are ketoconazole and caffeine. Studies using ketoconazole shampoo 2% (rather than the 1% available online) on androgenetic alopecia in men (MPB) revealed an augmentation in hair density as well as an increased size and proportion of anagen follicles when compared to those using a nondedicated shampoo (reference). A possible mechanism for this finding is topical ketoconazole’s suppression of androgen receptor activity.
Caffeine has potent antioxidant properties and has been identified as a stimulator of human hair growth in vitro, most likely due to inhibition of 5-α-reductase activity (reference).
When Medication is Not Enough
Fortunately, for many patients with hair loss for which medical therapy is not completely effective, advances in surgical techniques make hair transplantation a reliably effective option. The perfecting and worldwide adoption of modern techniques (see FUT, FUE, and scarless surgery) yields natural-appearing results that were not possible until approximately 5-10 years ago. Improvements in the surgical approach now allows many female patients, as well as men in the early stages of MPB, to benefit from this procedure. Furthermore, previously ‘pluggy’ transplants (seen in patients who chose to address their hair loss surgically prior to the evolution of current techniques) can now often be effectively repaired to make them appear natural.
Primary Sources:
- Dill-Muller D, Zaun H. Topical treatment of androgenetic alopecia with spironolactone. J Eur Acad Dermatol Venereol. 1997 Sep;9(Suppl 1):31.
- Kim JH, Lee SY, Lee HJ, Yoon NY, Lee WS. The Efficacy and Safety of 17α-Estradiol (Ell-Cranell® alpha 0.025%) Solution on Female Pattern Hair Loss: Single Center, Open-Label, Non-Comparative, Phase IV Study. Ann Dermatol. 2012 Aug;24(3):295-305.
- Fischer TW, Trüeb RM, Elsner P, et. al.Topical Melatonin for Treatment of Androgenetic Alopecia Int J Trichology. 2012 Oct-Dec; 4(4): 236–245.